














Recession caused by hard brushing pushed gums away from bridge margins
We will cover all the aspects, so you have a good idea of fair pricing for Gum Surgery when going abroad. What to look for, what to watch out for, and how to find the best provider for your case.
Gum recession is a condition where, as the name implies, the gum tissue recedes or becomes disconnected from the teeth. The most common cause of this condition is gingivitis, however there are also others such as a aggressive brushing, smoking, poor oral hygiene, bruxism, genetics, chronic diseases such as diabetes, periodontal disease and hormonal imbalances.
The receding gums causes sensitivity of the teeth, because the root of the tooth is exposed, and this contains extremely sensitive nerves. Discomfort can be caused by irritation, infection, or inflammation. To alleviate the symptoms of gum recession, the intervention of a periodontist is necessary to restore the appearance and function of the tissue.
If the plaque is not taken care of and continues to accumulate, bacteria may begin to grow and this will cause the gingivitis infection. There are many symptoms of gingivitis; these include bleeding, swelling, inflammation, and also a deep red color of the gums. Treatment of gingivitis depends on how severe and how far the disease has progressed. If gingivitis is not severe, the dentist could treat it with fluoride rinse and toothpaste to remove the plaque. Gingivitis that is not treated can lead to periodontitis and plaque, will spread and form underneath the gums. In plaque, the toxins made from the bacteria bother the gums. From support of the tissues and bone for teeth, they are broken and shattered.
In the procedure, Teeth will be separated from the gums and have spaces between them which are infected. As periodontitis continues, the bone and gum tissue are no long available. Hardly there are symptoms for this disease so, if patient doesn’t treat it, the teeth become useless and you will need an extraction. Gum disease treatment usually include professional dental cleaning, scaling, fluoride rinse and use of antibiotics. However, if the disease has progressed and spread deep under the gums and into the bone, surgical methods may be needed. Depending on the severity, surgical treatments include, bone and soft tissue grafts or even bone surgery. The best treatment method is always prevention.
GUM SURGERY COST IN MEXICO (Price Per Tooth)
Since its introduction to dentistry in 1994, Allo-Derm® Regenerative Tissue Matrix (RTM) has been a widely accepted acellular dermal matrix (ADM) for soft tissue applications. Allo-Derm® RTM supports tissue regeneration by allowing rapid revascularization, white cell migration and cell population – ultimately being transformed into host tissue for a strong, natural repair. (Thickness ranges from 0.9-1.6mm). AlloDerm is an acellular dermal matrix derived from donated human skin that undergoes a multi-step proprietary process that removes both the epidermis and the cells that can lead to tissue rejection.
AlloDerm is ideal for treating multiple defects in a single procedure.
Available sizes include: 1cm x 1cm, 1cm x 2cm, 1cm x 4cm and 2cm x 4cm.
After hydration it may be trimmed to the desired size with a scalpel or sharp scissors.
AlloDerm can be used effectively for soft tissue ridge augmentation. A tunnel or pouch may be created beneath the defect into which the AlloDerm can be inserted. If multiple layers of AlloDerm are used for increased thickness, it is recommended that it be layered, rather than rolled. In this indication, orient the dermal surfaces on the outside of the graft.
AlloDerm is effective in augmenting thin tissue around dental implants to create more attached tissue.
Eliminates the need for palatal surgery Removes palatal harvesting limitations from treatment planning considerations Reduces patient reluctance to follow through with surgical treatment Consistent quality Provided in multiple convenient sizes Available in two thickness ranges for use in different procedures: 0.9 to 1.6 mm – AlloDerm for root coverage, soft tissue ridge augmentation, etc. 0.5 to 0.8 mm – AlloDerm GBR for guided bone regeneration and barrier membrane function.
AlloDerm provides a matrix consisting of collagens, elastin, vascular channels, and proteins that support revascularization, cell repopulation and tissue remodeling. After placement, the patient’s blood infiltrates the AlloDerm graft through retained vascular channels, bringing host cells that adhere to proteins in the matrix. Significant revascularization can begin as early as one week after implantation. The host cells respond to the local environment and the matrix is remodeled into the patient’s own tissue, in a fashion similar to the body’s natural tissue attrition and replacement process. Because the components remain in their natural biologically active state, ADM is immediately recognized as human tissue.
AlloDerm has a safety history of more than a decade. Introduced in 1994 for treating burn patients, AlloDerm has proved its versatility and safety in more than a million diverse procedures in general, orthopedic, urogenital, and dental surgeries.
AlloDerm owes its exemplary safety to the safeguards at every step starting from donor screening to the final packaging.
The proprietary processing to derive AlloDerm from donor tissue involves a series of steps:
As described by Edward P. Allen, DDS, PhD and Lewis C. Cummings, DDS, MS
Treating multiple tooth recession defects traditionally requires a significant palatal tissue harvest to adequately supply enough donor material to successfully treat the defect. This often can lead to undesired surgical and post-surgical sequelae for both the surgeon and the patient. AlloDerm® RTM can be used as an effective alternative to palatal tissue in a wide variety of intraoral applications. 4 The following is an example of a suggested surgical technique for treating recession defects around teeth and dental implants. This technique can be modified to be applicable to the specific scenario being presented.
AlloDerm® RTM can be used as an effective alternative to palatal tissue in a wide variety of intraoral applications. 4 The following is an example of a suggested surgical technique for treating recession defects around teeth and dental implants. This technique can be modified to be applicable to the specific scenario being presented.
Begin with thorough root planing and root surface biomodification as determined by the surgeon and based on prior training and experience.
The pouch preparation begins with making papillary incisions approximately 3mm apical to the tip of the papilla between the lateral and canine and between the two premolars, leaving the papilla between #11 and #12 intact.
Leaving every other papilla intact helps prevent flap retraction and will improve the blood supply to the underlying graft.
Denude the remaining facial papillary tissue coronal to the incised papillae to serve as a recipient site for flap advancement.
Using an End-Cutting Intrasulcular Knife or similar microsurgical instrument, make sulcular incisions around each tooth with recession defects, as well as one additional tooth mesially and distally to facilitate flap mobilization.
A microsurgical elevator is used to lift the tunneled papillae and elevate a mucoperiosteal pouch just past the mucogingival junction at each tooth with recession as well as an additional tooth mesially and distally
Using a Modified Orban Knife, sharp dissect immediately supraperiosteally to mobilize and extend the pouch 12-15mm apical to the gingival margin at each tooth with recession as well as an additional tooth mesially and distally.
Separate the tunneled papillae from the interdental bone crest using a Younger-Good curette or similar instrument. Extend this blunt (supraperiosteal) elevation to the palatal/lingual line angles.
Trim the graft to extend from the distal of the central incisor to the mesial of the molar, with a vertical dimension of 8 mm. The graft is inserted into the pouch preparation under the tunneled papilla using a Younger-Good curette or similar instrument. Orient the graft with the reticular (connective tissue) side facing bone.
The graft should be positioned to extend from the distal of the central incisor to the mesial of the molar so that it lies completely under the papillae mesial and distal to the teeth with recession.
Place individual sling sutures around each tooth engaging the graft at the root line angles. The suture should be tied with the knot positioned palatally. The recomme ded suture is a 6-0 monofilament polypropylene.
The graft should not extend coronal to the cementoenamel junctions (CEJs) nor over the papillary vascular beds.
Place individual sling sutures around each tooth engaging the overlying tissue at the root line angles, 3 mm from the tissue margin without engaging the graft. You may place the micro elevator between the overlying tissue and the graft to prevent inadvertent engagement of the graft. The knot is positioned facially. Use the same 6-0 monofilament polypropylene suture.
Ideally, the graft should be completely covered. Exposure of 1 mm or less should not impact the outcome.
Each incised papilla should be secured by placing a suture through the papilla, passing through the embrasure, engaging palatal/lingual tissue, passing back through the embrasure and tying facially.
Surface sutures are removed at 4 weeks postop and the graft sutures are removed at 2 months post -op. Complete root coverage in Miller Class l and ll recession with an increase in marginal tissue thickness and stability should be achieved.
More dentists and patients are becoming aware of receding gum tissue. What is this all about? How does it start? Why is gum recession a problem? Can recession be prevented? Can recession be reversed and repaired? What are the different types of treatment for gum recession? Since the management of gum recession is evolving yearly with attempts with different styles and treatment techniques, we'd like to provide a knowledge base that can allow you to understand the rationale of our approach of treatment. We will acknowledge that since treating and preventing gum recession is a significant part of our practice, Mexican dentists have refined theirs techniques to a degree that the approach can vary from standard treatment approaches provided by many talented and competent periodontists.
If there is adequate pink gingiva around the tooth and if there are no other conditions that challenge its integrity such as excessive tooth brushing, tobacco use, gum inflammation (gum disease) or irregular tooth position, the gum line can stay at its natural position for a lifetime. Even with aging, one does not need to have recession or be “long-in-the-tooth”.
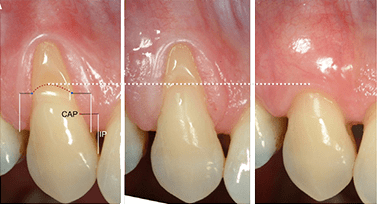
When circumstances cause thinning or irritation to the gums, they can get either worn away and degenerate if the blood supply to the gum line becomes compromised. This can also occur as a consequence of inflammatory gum disease called periodontitis. Whether by inflammation, irritation, or other causes, the gums can break down and expose the root of the tooth. The tooth root has a different makeup than the top or crown of the tooth. While the top of the tooth which we’re used to seeing is covered with a highly calcified dental enamel, the root is much softer and is covered with a thin layer of less calcified structure called cementum under which is the body of the tooth root made of dentin. Again, dentin is much softer than the enamel that covers the crown of the tooth. As the tissues descend along the root surface giving the appearance of receding gums, the bone around the tooth that holds the tooth in place is descending along with the gum tissue.
Dense calcified tooth enamel Softer(less calcified) tooth root surface Periodontal (gum) recession: Loss of gum tissue and bone covering the tooth root No protective pink gingiva below recession
No treatment to repair gum tissue and reverse recession will be successful if the cause of the recession is not addressed. Some contributing factors for recession don’t relate to behavior and some factors can be modified by behavior.
However, many cases of periodontal recession have been contributed to by toothbrush abrasion, or simply brushing too hard. This can occur whether you use a manual or a power toothbrush. Well-meaning parents often taught children to “scrub” their teeth, but scrubbing teeth and gums often wears away the gum tissue and even cuts grooves into the roots of teeth. As these “scrubbing” kids grow up, a sense of well-being occurs with harsh brushing so that the irritation of brush makes teeth “feel clean”.This is a case of harm being caused by too much of a good thing.
Add lots of toothpaste to the harsh brushing and the abrasion is made even worse. Most commercial toothpastes contain abrasives that can add to the abrasion, especially if used in large amounts. Are you a hard brusher? One way of testing if you brush too hard is to look at your toothbrush. If brushing correctly, a normal tooth brush should last at least 3 months. It can be replaced when the bristle begin getter soft or lose their resiliency. However, the toothbrush bristles should look just like the way you bought it. If you find the bristles are getting flattened or pointing in all directions of the compass, you’re brushing too hard. An objective test to determine if there is toothbrush abrasion is to look at toothbrush wear. If used properly, your toothbrush bristles should look new after 3 months of use. If bristles are matted down or splayed, you’re brushing too hard. A good way to prevent abrasion is to hold the brush with fingertips only. At first it feels strange! But it works!
Recession caused by hard brushing pushed gums away from bridge margins
Recession caused by hard brushing affected several teeth in a row
Recession caused by hard brushing were “repaired” by white fillings instead of moving gums back into natural position
Breaking the hard brushing “addiction” is difficult and gentle brushing won’t feel very good – at first. At first, you won’t believe you can really get your teeth clean by gentle brushing, but you can. Once you get used to being comfortable without the irritation, you’ll be “home-free”! Give yourself lots of time to practice gentle brushing, and don’t give up! Start by holding your toothbrush with your fingertips. It doesn’t matter if you use a manual or power brush, you are no longer going to use the “full-fisted death-grip”.
Smoking causes irritation to gum tissue that increases the risks for recession.
While the idea of smokeless tobacco seems to give comfort that derails the possibility of lung cancer, any tobacco products that are used or held in the mouth irritates the oral tissues to a level that can cause oral cancer.
The irritation of tobacco being held in the mouth between the cheek and gums is especially harmful to the gum tissue and contributes directly to choking off gum tissue resulting in recession of periodontal tissues.
Yes, orthodontic straightening of the teeth will make you pretty, but often lost in the discussion is how straight teeth can help you keep your teeth. Many crooked teeth that lean toward the lips and cheek develop very thin gums or actual recession of the periodontal tissues because they are moving away from the jaw bone and the tissues that cover the teeth.
Also, crooked teeth can’t rely on support of neighboring teeth to keep them in place so crowded teeth will get more crowded with passing years. Orthodontists are now skilled at correcting these problems for adults.
With an aging population that will need good nutrition in later years, having teeth in the right position will help keep them in the mouth where they do the most good.
We help you to find a dentist in Mexico. Free Dental Tourism Advice.
For some people, there is not enough protective gum tissue (gingiva) around the teeth, making the teeth prone to periodontal (gum) recession. This gingiva can sometimes be so thin it appears to be like wet tissue paper over teeth. In cases such as this where existing gum tissue is threatened, a soft tissue (gum or gingival) graft is recommended to thicken or fortify the gingiva. This increase in thickness makes the tissue stronger and more resistant to irritation.
The term “free” indicates that gingiva from another site within the person’s mouth (donor site) is “freed” or lifted off its base and then moved and secured with stitches to the site where new tissue is needed (recipient site). The procedure involves only superficial tissues (a few millimeters) requiring only local anesthesia. Search the internet, speak with other periodontists, consult with dental school professors and they will state that the donor tissue for free gingival grafts comes from the roof of the mouth (palate). This has been the standard approach since the procedure was developed in the 1960’s and tissue from the palate does work well. Despite its predictability, the surgical wound from the roof of the mouth is often quite painful, both by injection of the palate with anesthetic and the discomfort during the first week of healing. To assuage the discomfort, dressings are applied to the roof of the mouth with or without a plastic appliance or “stent” that protects the palate. The discomfort can require pain medication and sometimes bleeding is a problem.
However, there is a different way of doing the free gingival graft that has being developed and tested in different offices that believe is more comfortable and has a better appearance after healing. The majority of patients have plenty of sound donor gum tissue on outside gum tissue (gums that face the lips and cheeks) that can be used with no damage to the donor site. In fact, these sites can be repeatedly “harvested” if necessary. Using this alternative location offers much improved comfort with no need for injections or wounds on the roof of the mouth. Additionally, since the outside gum tissue has the same character of the tissue that is desired in the graft, the non-palatal graft often “blends” better visually with surrounding tissues compared to grafts using the palatal tissue which often have a lighter color than adjacent tissues.
They work to help prevent recession, but they are too large (most people do well with a moderate amount of protective gum tissue [gingiva]), they graft areas that don’t need grafting, and one can unpleasantly imagine how much tissue must have been taken from the roof of the mouth and the likely discomfort that accompanied the wound on the palate. Most periodontists do much better than these, but they show the typical color difference between tissue from the roof of the mouth and the color of natural gum tissue (gingiva). The majority of patients have plenty of sound donor gum tissue on outside gum tissue (gums that face the lips and cheeks) that can be used with no damage to the donor site.
How can we repair gums that have already receded? For many years, reversing recession and restoring gums to their natural position was an unpredictable affair. Failure to cover roots led many periodontists to abandon any attempt to do so. In fact, many general dentists are just learning about the increased predictability of covering exposed tooth roots. Rather than put fillings in decayed, worn, or discolored exposed roots or covering the roots with long porcelain crowns, dentists are now providing patients with the opportunity to “turn the clock backwards” and restore the gums back to their original position through gum grafting.
The conventional and standard method of correcting recession when the existing gum tissue is thin or absent is to perform a 1-Step procedure called a sub-epithelial connective tissue graft. Phew! What a term! As with the free gingival graft, nearly all periodontal residencies and dental schools use this as the standard technique for correcting periodontal recession. This highly successful procedure has the operator take tissue from under the skin of the roof-of-the-mouth (called connective tissue). This tissue is then lifted away and the connective tissue is placed under a flap of tissue that is loosened and moved over the connective tissue and receded root. The root is prepared by cleaning and sometimes treated with medications intended to help the soft tissue adhere to the roots. Stitches (sutures) are used to secure the flap and connective tissue in place. An alternative tissue that can be used is freeze-dried human skin that is used in place of the connective tissue which avoids the palatal donor site
For patients with lots of good gum tissue that are receded, we often use the coronally advanced graft: This surgical procedure simply loosens the existing gum tissue by teasing it off the underlying hard tissue (bone) making it “movable”. By loosening it just enough, the gum tissue can be placed over the receded root like a window shade. Once in its desired position, a tiny suture (stitch) similar to a thickness of hair secures the tissue in position by weaving it between the teeth. One advanced technique we often use keeps all the gums intact while we loosen it. This means that there is minimal incision of the gums. Most of the loosening is done through the gum line and most tissue between the teeth remains intact. This preservation of the papilla, or the gum tissue between the teeth helps healing and prevents deforming this important tissue. If teeth are too close together, the papilla might be too fragile to keep it together or the surgeon may use a different technique is appropriate, but special care is taken to minimize hurting this “pointy” tissue between the teeth. Complicating factors can be poor contours of gum tissue, crooked or rotated teeth, and tooth crowding that compress the tissue these papillae that carry nutrients to the gum tissue. Some dentists would put fillings on the discolored roots and cover the teeth and roots with crowns More dentists are now aware that rather than patch the teeth, restoring the natural condition of the gums and teeth is a practical option.
In this procedure developed in our practice, a single treatment can now be done to achieve two goals. Conventional soft tissue graft therapy offers: Predictable increase in protective pink gingiva with a free gingival graft. Predictable coverage of tooth roots exposed by periodontal recession with a range of grafts including use of palatal connective tissue or other material such as freeze dried human skin (allograft). However, neither of these procedures can routinely cover roots and add true gingiva in a single procedure with predictability. The SimulGraft was developed and is being refined by Dr. Simonds in 2014 and was presented to the American Academy of Periodontology in 2015. The SimulGraft simultaneously expands the band of true pink gum tissue (gingiva) on a tooth or teeth and covers the tooth root exposed by periodontal recession. This is all done while using no tissue from the roof of the mouth (palatal donor tissue) and consequently avoiding any risk of palatal pain, bleeding, or need for healing treatment on the roof of the mouth. The SimulGraft combines the predictability and minimal invasiveness of the non-palatal free gingival graft with coronally advanced (tissue moved over the root) graft. While continuing to be studied and evaluated, the confidence level achieved with this procedure is at such a level that the SimulGraft is now our primary recommendation for patients with both mild to moderate periodontal recession and lack of protective pink gum tissue (gingiva).
Unlike conventional sub-epithelial connective tissue grafts that are usually taken from the roof of the mouth, the SimulGraft uses a thin piece of gum tissue from common sites on outside gum tissue such as the triangular tissue between the teeth. This tissue heals back without damaging the site. In rare instances where there is insufficient non-palatal tissue available, the palate remains a donor tissue option. The SimulGraft uses the patient’s own tissue and does not require an alternative of taking cadaver skin from a tissue bank. While standard procedures have good predictability, it can often happen that no new pink gingiva is created by the graft. The SimulGraft predictably adds this pink tissue to the treatment site. We feel the pink gingiva restores the natural protective structure of the gum tissue and also provides natural appearing tissue.
Like the standard palatal connective tissue graft of the grafts using cadaver skin, SimulGraft covers many types of periodontal recession predictably. The SimulGraft was developed to treat one or multiple teeth in a single visit similarly to connective tissue grafts, but without any disturbance to the roof of the mouth
In situations of severe periodontal recession where predictable root coverage with regeneration of pink gums (gingiva) without using the roof of the mouth cannot be reasonably achieved with the 1-Step SimulGraft, a 2-Step Non-Palatal approach is often a good option. Conventional soft tissue graft therapy offers: predictable increase in protective pink gingiva with a free gingival graft. predictable coverage of tooth roots exposed by periodontal recession with a range of grafts including use of palatal connective tissue or other material such as freeze dried human skin (allograft). However, neither of these procedures can routinely cover roots and add true gingiva in a single procedure with predictability. The 2-Step approach increases predictability by performing 2 more predictable procedures sequentially.
There is usually a recommended 1-2 month waiting period between treatment stages. The waiting time may be longer between stages since there is more protective tissue after Step-1 that should protect the site from further recession In Step-1, a site with periodontal recession and inadequate protective gingiva is treated with a free gingival graft to increase the amount of sound gingiva. In the procedure, donor gingiva is “freed” up from a separate site in the mouth (we usually avoid using the palate) and grafted into the site that needs the extra tissue. The free graft is one of the most predictable procedures in periodontics. Occasionally, some of the periodontal recession can be reduced with the free graft depending on certain conditions. In Step-2, the newly grown gingiva is loosening from its base and drawn over the tooth root exposed by periodontal recession. If there is sound gum tissue between the teeth and if other conditions are favorable, much of the exposed root can be covered. With proper care this treatment can be long lasting.
Unlike conventional sub-epithelial connective tissue grafts that are usually taken from the roof of the mouth, the Step-1 procedure uses a thin piece of gum tissue fromcommon sites on outside gum tissue such as the triangular tissue between the teeth. This tissue heals back without damaging the site. In rare instances where there is insufficient non-palatal tissue available, the palate remains a donor tissue option.Like the SimulGraft, the 2-Step Approach uses the patient’s own tissue and does not require an alternative of taking cadaver skin from a tissue bank. While standard procedures have good predictability, it can often happen that no new pink gingiva is created by the graft. The 2-Step Approach predictably adds this pink tissue to the treatment site to a degree even greater than the SimulGraft. We feel the pink gingiva restores the natural protective structure of the gum tissue and also provides natural appearing tissue. Like the standard palatal connective tissue graft or the grafts using cadaver skin, both the SimulGraft and 2-Step Approach covers many types of periodontal recession predictably. Like the increased predictability of the 2-Step Approach in rebuilding gingiva, it also has enhanced predictability to cover exposed roots. The SimulGraftTM was developed to treat one or multiple teeth in a single visit similarly to connective tissue grafts, but without any disturbance to the roof of the mouth. As suggested in the name, the 2-Step Approach does require two surgical treatments. The benefit of the 2-Step Approach is the increased predictability of both creating new gingiva and achieving maximum coverage of exposed by periodontal recession compared to other techniques including the SimulGraft
Just like the Non-Palatal Free Gingival Graft used to prevent recession described before, a site with periodontal recession and little or no gingiva first is treated to add more gingiva. This 1st Step graft: 1. Adds protective tissue that will protect and stabilize the gum line. 2. Provides a known amount of gum tissue that will used to cover the recession in the 2nd Step procedure. This reduces guesswork.
Just like the Non-Palatal Free Gingival Graft used to prevent recession described before, a site with periodontal recession and little or no gingiva first is treated to add more gingiva. Once the “new” protective gum tissue (gingiva) is added by the 1st Step graft, the receded tissue is now thicker, stronger and more resistant to future irritation. The Step 2 procedure will now move this new healthy tissue into position to cover the root.
Within the next 2 weeks, skin cells will form a seal between the tooth root and gum tissue. After numbing, the exposed tooth root is cleaned, reshaped, or otherwise repaired (such as removing decay or old fillings) so it is prepared to accept the new gum tissue that will cover it. The gums to be moved are loosened by gently “teasing” them off the underlying tissues. This makes the tissues moveable like a loose fitting shirt.
Without making significant incisions or cutting papilla (the pointy gums between the teeth), most of this loosening is done through insertion of instruments under the gum line and through a small incision in the loose tissue next to the gums. After a week or two, skin cells work their way between the gum tissue and the root and form a seal between them. If well cared for, this seal can function and be a successful long-term treatment.
Severely receded tissue with no pink gums (gingiva)
Step 1 Complete: New pink gingiva added above recession to thicken the gums
Step 2 Complete: New pink gingiva is moved to cover recession
When there is sufficient protective gum tissue next to a site with inadequate gum tissue (gingiva) and recession, the area “next door” can serve as the donor site for the graft. A preparation is made in the numbed recipient site (where the graft will be placed) while the tissue is lifted from the donor site, leaving the graft attached at its base. Recession and thin tissue next to the tooth with ample gum tissue.
The donor tissue is “swung” over to cover the recession bringing with it the sound gingiva needed at the site of recession. The advantages of this type of graft include not needing extra tissue from another site and it will usually provide a better color match to the grafted site compared to a graft that comes from the roof of the mouth.
Also, since the lateral graft is not totally freed from its base, it retains part of its nutrient supply. This improves the chances for a successful graft and provides improved possibilities for covering the root surface exposed by the recession. Because there is just one surgical site, these grafts are often quite comfortable during healing.
In the confusing marketplace of dental treatment, how can patients make informed choices? Each practitioner has his or her technique that works the best for them. Depending on the focus of the practice, some periodontists commit more or less time treating recession lesions and develop different expertise in certain procedures. Below is a chart of some of the techniques available today and compares some of the features.
Each patient who wants to make an informed decision on which procedure to choose can highlight features that are most important and use these as discussion points before treatment is performed.
Check out the clinics listed on our website, here you will find the best-ranked periodontists in Mexico. Review and investigate their Credentials and continuing education, search dentists with before and after pictures, or reviews to know theirs work. During negotiation ask the periodontist if he accepts Dental insurance plans, it could help you to save even more money. Make sure dental facilities have state-of-art technology, it also has a large impact on the quality of dental work.


